




10 min read
Movement coaches, physical therapists, and fitness professionals often focus on the more visible or commonly discussed joint actions like flexion, extension, or rotation. However, understanding the subtler movements of scapular elevation and depression, along with their associated muscle activity, is crucial for optimal shoulder function, injury prevention, and athletic performance.
A thorough understanding of the anatomy, structure, and function of the scapula is essential, as it allows for optimal movement and helps prevent injuries by ensuring both anatomical integrity and proper biomechanics.
“The scapula is the foundation upon which all upper extremity movement is built. Ignore it at your peril.”-Dr Ben Kibler, renowned shoulder specialist
This comprehensive guide explores the anatomical foundations, functional applications, and coaching cues for elevation and depression movements of the scapula (shoulder blade). The ligaments associated with the structure of the scapula underpin its function in upper extremity movement, making it vital to assess both aspects for effective training and rehabilitation.
What Are Scapular Elevation and Depression?
Let’s start with clear definitions:
Elevation refers to the upward movement of the scapula, such as when you shrug your shoulders. Depression is the opposite movement, like when you lower your shoulders after a shrug. These movements occur at the scapulothoracic articulation and are closely related to the function of the shoulder joint and other joints of the upper limb.
The relationship between elevation and depression is facilitated by the coordinated action of several joints, including the shoulder joint, which allows for smooth and controlled movement of the scapula.
Elevation Movement
Elevation movement refers to the upward movement of the scapula. The acromion and acromioclavicular joint are key anatomical landmarks involved in scapular elevation. Think of shrugging your shoulders toward your ears; that’s scapular elevation in action. This movement is critical in various activities, from reaching overhead to certain phases of throwing motions.
Depression of the Scapula
Depression of the scapula(or shoulder depression) is the opposite movement, drawing the shoulder blades downward, away from the ears. The impact of gravity assists in the downward movement of the scapula during depression, making it a passive force that influences scapular alignment. This action is essential for postural control and serves as a foundation for many upper-body exercises.
The relationship between these movements creates a balanced shoulder girdle that can efficiently transfer force between the trunk and upper limbs. The angle of the scapula, particularly the position of the superior angle relative to the thoracic spine, can be assessed to determine if scapular depression is excessive or within normal limits.
Muscles Responsible for Scapular Elevation and Depression
Understanding the muscles that control these movements is essential for targeted training and rehabilitation. The function of these muscles depends on proper innervation by specific nerves, which control muscle activation and coordination.
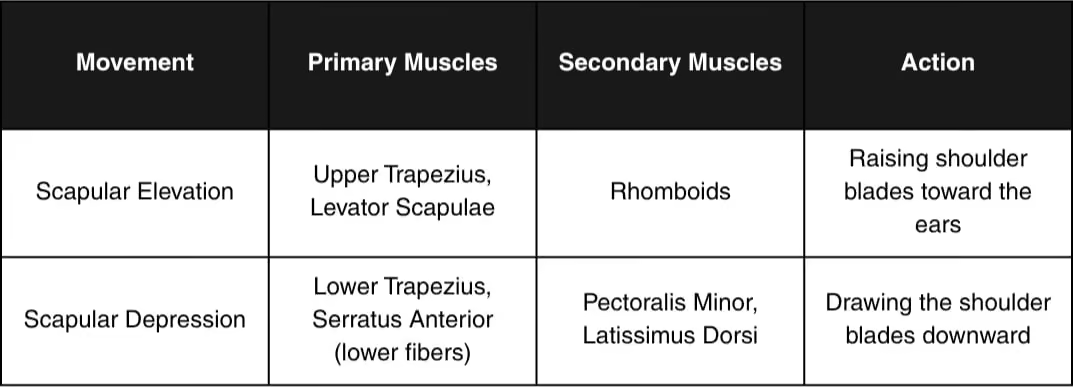
Scapular Elevation Muscles
The primary muscles responsible for the forelevation of the shoulders include:
- Upper trapezius (also known as the upper traps) - The most powerful elevator of the scapula
- Levator scapulae - As its name suggests, it elevates the scapula
- Rhomboids (minor and major) - Assist in elevation while also retracting
In addition to these muscles, ligaments such as the acromioclavicular and coracoclavicular ligaments help stabilize the scapula during elevation.
Scapular Depression Muscles
The muscles that depress the scapula include:
- Lower trapezius- Primary scapular depressor
- Serratus anterior(lower fibers) - Assists in depression while also contributing to upward rotation
- Pectoralis minor- Pulls the scapula anteriorly and downward
- Latissimus dorsi- Although primarily acting on the humerus, it can influence scapular depression and also assists in adduction of the arm
The biceps brachii, while not a primary depressor, originates from the scapula and plays a role in shoulder stability.
Why Scapular Elevation and Depression Matter
The ability to properly control elevation and depression anatomy movements has significant implications for:
1. Posture
Chronic elevation of the shoulders is a common postural dysfunction. Ideally, the middle border of the scapula should align parallel to the thoracic spine, with the level of the scapula's middle portion near the 2nd thoracic vertebra for optimal posture. Learning to engage the scapular depression muscles helps establish a more neutral shoulder position, reducing strain on the neck and upper back.
2. Shoulder Health
“The scapula must be able to freely move through depression and elevation to accommodate the humeral head during arm movements. Restriction in either direction can lead to impingement and pain.”- Dr. Shirley Sahrmann, movement science expert
The rotator cuff muscles play a key role in maintaining shoulder health and preventing impingement by stabilizing the shoulder joint and supporting proper scapular movement.
Proper scapular positioning through balanced elevation vs depression control is critical for maintaining the subacromial space and preventing impingement syndromes. Appropriate treatment strategies are essential for addressing impingement and restoring normal scapular movement.
3. Athletic Performance
Many athletic movements require coordinated elevation and depression movements:
- Throwing athletes need controlled elevation during the cocking phase
- Swimmers utilize scapular depression for powerful pull phases, often performing scapular depression during each stroke
- Weightlifters must stabilize through depression during heavy pressing movements
Sports med approaches often focus on optimizing scapular control in athletes to enhance performance and prevent injury.
4. Breathing Mechanics
The accessory breathing muscles include many of the same muscles involved in scapular elevation. Understanding this relationship helps in addressing breathing pattern disorders.
Assessing Scapular Position and Movement
Before prescribing exercises, coaches should assess scapular positioning and movement patterns. Determining the underlying causes of abnormal scapular positioning is essential before intervention to ensure effective and safe treatment.
Common Dysfunctions
- Elevated Shoulder Posture (Shoulder Elevation) Appearance: Shoulders perpetually shrugged
- Associated with: Neck pain, headaches, upper trapezius dominance
- Often seen in: Desk workers, individuals with high stress
Depressed Shoulder Posture (Excessive Scapular Depression)
- Appearance: Shoulders appear pulled down and forward
- Associated with: On the affected side, thoracic outlet symptoms or breathing restriction may be present
- Often seen in: Some athletes with overdeveloped lats, military postures
Assessment Tests
The shoulder depression test is one method to assess control and strength in the depressing musculature. This clinical procedure is used to evaluate scapular control and identify any dysfunction:
- Have the client stand with arms at their sides
- Ask them to actively draw their shoulder blades down (without shrugging or excessively retracting)
- Observe for symmetry and control during the movement
- Apply gentle resistance to test strength
Best Exercises for Scapular Elevation and Depression
Elevation Training Exercises
- Shoulder Shrugs: Simple but effective for training, scapular elevation
- Can be performed with or without weights
- Focus on the full range of motion and controlled tempo
Y-Raises
- Combining elevation with upward rotation
- Excellent for training proper overhead movement patterns
Exercises for Depression of the Scapula
- Scapular Pull-Downs
Stand or sit tall - Without moving your arms, draw your shoulder blades down away from your ears, performing the movement with attention to scapular positioning and approximately 30° of internal rotation for optimal biomechanics.
- Hold for 5 seconds, then release
- Perfect for learning to depress the scapula muscles while considering medial rotation and lateral rotation of the shoulder joint during exercise design.
Band Pull-Aparts with Depression
- Hold a resistance band at shoulder height
- As you pull the band apart, simultaneously depress your shoulder blades, performing the movement with proper scapular alignment.
- Emphasizes scapular depression with retraction
Lat Pull-Downs with Scapular Emphasis
- Focus initially on depressing shoulder blades before bending elbows, performing the exercise with awareness of internal rotation for optimal shoulder stability.
- Teaches proper sequencing of scapular and glenohumeral movements
Push-Up Plus with Depression
- At the top of a push-up, push further to protract the scapulae
- Then actively depress the scapulae without retracting, performing the movement with attention to scapular internal rotation.
- Excellent for serratus anterior and lower trapezius coordination
Clinical Relevance of Scapular Dyskinesis
Scapular dyskinesis refers to altered scapular position and motion. It’s often associated with various shoulder pathologies and can manifest as either excessive or restricted elevation and depression movement.
For a comprehensive overview of current knowledge on scapular dyskinesis, including clinical management and pathophysiology, see the narrative review published in BMC Musculoskelet Disord.
What does scapular dyskinesis feel like?
Patients typically describe:
- A feeling of “winging” or the scapula sticking out
- Clicking or grinding sensations during arm movements
- Fatigue in the shoulder region
- Limited range of motion overhead
What does scapular pain feel like?
Scapular pain often presents as:
- Dull ache between the spine and scapula
- Sharp pain with specific movements
- Referred pain into the upper arm or neck
- Pain that worsens with prolonged positions
Why does it feel like my shoulder blade is sticking out?
This sensation, often described as scapular winging, can result from:
- Weakness in the serratus anterior muscles
- Nerve dysfunction (particularly the long thoracic nerve; the brachial plexus may also be involved in some cases)
- Imbalance between protractors and retractors
- Poor motor control of the scapula during movement
Rehabilitation Strategies
How to release tension in the scapula?
Techniques to address scapular tension include:
- Soft Tissue WorkFoam rolling upper back
- Targeted massage for the upper trapezius, levator scapulae, and rhomboids
- Lacrosse ball techniques for the serratus anterior
Stretching
- Upper trapezius stretches (for chronically elevated postures)
- Pectoralis minor stretches (for the for anterior depression of the scapula)
- Latissimus dorsi stretches (for restricted elevation)
Breathing Exercises
- Diaphragmatic breathing to reduce accessory muscle dominance
- Lateral costal breathing to improve rib mobility
How to correct a depressed scapula?
Each patient may require a tailored approach based on their specific presentation when addressing a chronically depressed shoulder position:
- Release tight depressors: Latissimus dorsi and pectoralis minor releases
- Lower trapezius trigger point work
Activate elevators
- Gentle upper trapezius and levator scapulae activation exercises
- Progressive loading of elevation patterns
Postural awareness
- Mirror feedback
- Taping techniques for proprioceptive feedback
“Rehabilitation isn’t about strengthening muscles in isolation—it’s about restoring balanced movement patterns. With the scapula, this means ensuring smooth coordination between elevation and depression forces.”
-Dr. Jill Cook, physiotherapy researcher
The ultimate goal is to restore optimal function to the upper limb by improving scapular mechanics and stability, allowing for a full range of motion .
Integration Into Training Programs
Coaches should consider the following principles when incorporating scapular elevation and depression work:
1. Begin With Awareness
Coaches should consider the following principles when incorporating scapular elevation and depression work, particularly when scaling programs across multiple clients. Platforms like FitBudd allow coaches to build standardized scapular control progressions, deliver exercise videos with precise cues, and monitor adherence—making it easier to reinforce awareness-based corrections consistently inside and outside the gym
- “Gently slide your shoulder blades down and back.”
- “Imagine your shoulders melting away from your ears.”
- “Create space between your shoulders and earlobes.”
2. Isolate Before Integration
Master basics, scapular depression, and elevation movement before adding complex patterns:
- Seated depression/elevation exercises
- Quadruped or prone scapular control work
- Standing exercises with arm movements
- Dynamic movements under load
3. Train Through Full Ranges
Develop control throughout the complete elevation depression anatomy spectrum:
- Scap depression at the end ranges
- Mid-range stability
- Controlled transitions between movements
4. Balance With Other Scapular Movements
Remember that depression/elevation are just two of the scapular movements. Integrate with:
- Protraction/retraction
- Upward/downward rotation
- Anterior/posterior tilt
Case Studies: Elevation and Depression in Practice
Case 1: The Desk Worker with Chronic Neck Pain
Presentation:
- Chronically elevated shoulders
- Weak lower trapezius
- Pain with prolonged sitting
Intervention:
- Regular scapular depression practice during the workday
- Lower trapezius strengthening
- Pectoralis minor releases
- Workstation ergonomic adjustments
Outcome:
- Reduced neck tension
- Improved posture
- Decreased pain frequency
Common Coaching Mistakes to Avoid
- Confusing Depression with Retraction. Scapular depression is a downward movement.
- Retraction is drawing the shoulder blades together
- They often occur together, but are distinct movements
Over-Cueing Depression
- Excessive shoulder depression can create new problems
- Balance is key—neither elevated nor excessively depressed
Ignoring Individual Variations
- Anatomical differences affect optimal positioning
- What looks “depressed” on one person may be neutral for another
Neglecting Other Movement Planes
- Focusing solely on elevation vs depression without addressing rotation
- All scapular movements must work in coordination
Red Flags and When to Refer
Understanding the innervation of the muscles involved, coaches should be aware of potential serious issues requiring medical attention:
What is a red flag for bilateral shoulder pain?
- Sudden onset of bilateral symptoms without a clear cause
- Neurological symptoms (numbness, tingling, weakness)
- Symptoms associated with breathing difficulties
- Pain unrelated to movement or position
What does a positive shoulder abduction test mean?
A positive test may indicate:
- Nerve root compression or irritation
- Cervical spine involvement
- Potential need for medical evaluation before continuing exercise
Conclusion
Mastering the concepts of scapular elevation and depression provides coaches with powerful tools for improving movement quality, enhancing performance, and preventing injury. By understanding the anatomical foundations, assessment strategies, and practical applications of these movements, you can better serve your clients and athletes.
Remember that balanced control of these movements, rather than fixed positions, is the goal. The scapula must be free to move through its full range while maintaining appropriate relationships with the thorax and humerus.
“The scapula is like the conductor of the shoulder symphony. When it moves with precision and timing, all other elements fall harmoniously into place.” - Gray Cook, physical therapist and movement specialist.
Implementing these concepts with your clients will not only improve their shoulder function but will also demonstrate your expertise as a movement professional who understands the subtleties that make a significant difference.
Frequently Asked Questions (FAQs)
1. What is scapular depression, and how does it differ from elevation?
Scapular depression refers to the downward movement of the shoulder blade, away from the ears, while elevation is the opposite movement, where the scapula moves upward. Both are essential scapular motions for maintaining balance and mobility in the upper limb, especially during overhead or weight-bearing activities.
2. Which muscles control scapular depression, and how do the trapezius and serratus anterior contribute?
The lower trapezius and serratus anterior (lower fibers) are primary muscles involved in depression of the shoulder. The trapezius assists in stabilizing and pulling the scapula downward, while the serratus anterior helps control lateral rotation and maintain proper scapular alignment against the thoracic wall during movement.
3. Why is understanding the anatomy of the back of the scapula important in physical therapy?
The anatomy back scapula, including landmarks like the acromion and coracoid process, helps physical therapists assess scapular positioning, muscle imbalances, and potential dysfunction. Precise understanding aids in diagnosing issues related to the rotator cuff, postural problems, and impingement syndromes that affect the upper limb.
4. How do rotation movements of the scapula—medial and lateral—impact shoulder function?
Medial rotation (downward rotation) and lateral rotation (upward rotation) of the scapula are essential for full shoulder mobility. These movements are especially important when evaluating shoulder blade control in activities like lifting or reaching. Dysfunction in either direction can compromise muscle activity, contribute to pain, or affect the function of the rotator cuff and glenohumeral joint.
5. How do the acromion and coracoid process influence shoulder stability and movement?
The acromion and coracoid process are bony projections of the scapula that serve as attachment points for key ligaments and muscles. They play crucial roles in maintaining shoulder blade stability, supporting muscle activity during arm movement, and protecting structures like the rotator cuff and blood supply pathways from compression or injury.
6. How is scapular depression assessed or treated in physical therapy?
In physical therapy, scapular depression is assessed through posture analysis and movement tests. Treatment may include strengthening the lower trapezius, stretching tight upper traps, and activating supportive muscles like the serratus anterior. Techniques often address dysfunctional patterns such as chronic elevation, ensuring balance in the scapula’s mobility and muscle activity.
7. Can you give a case study involving scapular depression?
Case study: A swimmer presents with shoulder tightness and poor pull-through during strokes. Assessment reveals overactive latissimus dorsi and weak lower trapezius, causing excessive scapular depression and poor lateral rotation. Treatment focuses on strengthening the upper traps, improving rotator cuff support, and retraining scapular movement patterns with medial rotation control.
%20to%20Become%20a%20Certified%20Personal%20Trainer-min.avif)








