




10 min read
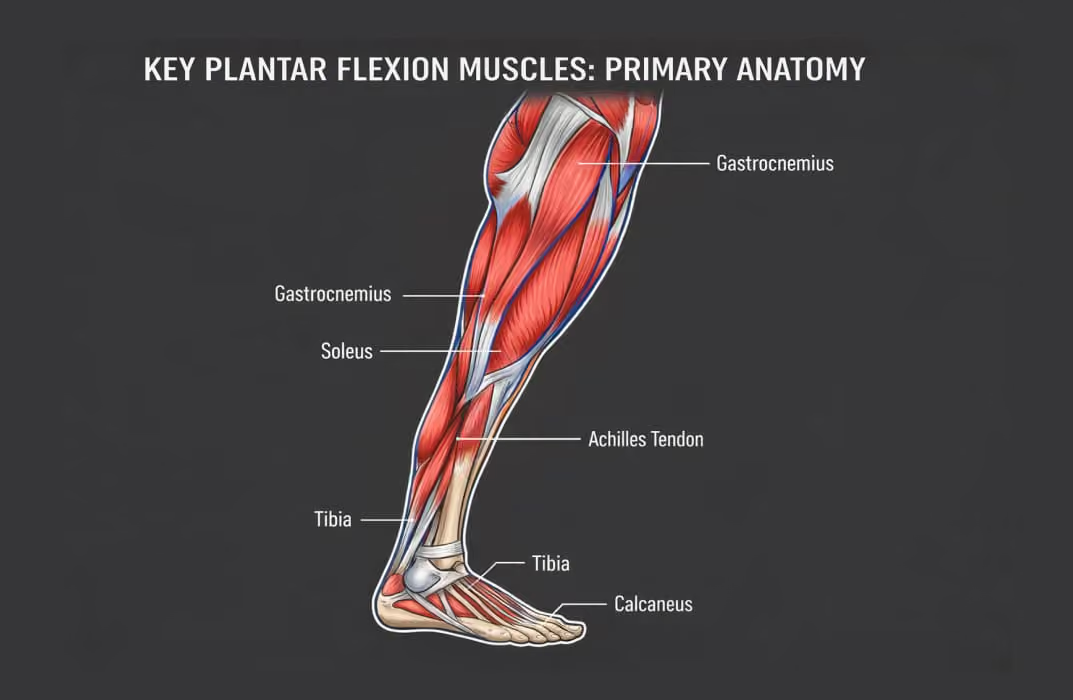
Plantar flexion is powered primarily by two muscles the gastrocnemius and the soleus working through the Achilles tendon, with the plantaris, tibialis posterior, flexor digitorum longus, flexor hallucis longus, and the peroneals adding secondary force. Together they drive one of the most-used movement patterns in the body: every time you walk, run, jump, cycle, climb stairs, or stand, you're using your plantar flexors. Yet despite that frequency, these muscles are among the most undertrained, poorly differentiated, and frequently injured in fitness populations and the imbalances between them sit behind a large share of the calf, Achilles, and ankle injuries coaches see.
The reason most coaches give insufficient attention to plantar flexor muscles is straightforward: these muscles are often loaded passively during compound lower-body exercises like squats, deadlifts, and lunges. Coaches assume sufficient calf training is occurring without realizing that these exercises primarily train the gastrocnemius, incidentally, and almost entirely neglect the soleus.
This has real consequences. Achilles tendinopathy is one of the most prevalent overuse injuries in active populations. Plantar fasciitis affects approximately 1 in 10 people at some point in their lives. Calf strains are the second most common muscle injury in team sport athletes. Most of these injuries are either directly caused or significantly worsened by plantar flexor imbalances that systematic assessment and targeted programming would have identified and addressed.
This guide provides coaches and fitness professionals with the complete picture: the precise anatomy of every plantar flexion muscle, how the gastrocnemius and soleus differ in function and fiber type, the role of each secondary muscle, the biomechanics of plantar flexion in movement, the most common imbalances and their downstream consequences, how to assess plantar flexor function, and evidence-based programming to train and correct each muscle group effectively.
How Does Plantar Flexion Work at the Ankle Joint?
Plantar flexion occurs primarily at the talocrural joint, the articulation between the talus (the uppermost bone of the foot) and the tibia and fibula of the lower leg. This joint functions as a hinge joint that moves primarily in the sagittal plane, allowing the foot to move upward (dorsiflexion) and downward (plantar flexion).
The normal range of motion for plantar flexion is approximately 40 to 50 degrees from the neutral position (foot at a right angle to the tibia). This range varies between individuals based on muscle flexibility, joint mobility, and tendon length. Athletes with very mobile ankles may achieve 60 degrees or more. Clients with chronically shortened calf muscles or prior ankle injuries may have significantly reduced plantar flexion range of motion.
The force of plantar flexion is transmitted through the Achilles tendon, the body's thickest and strongest tendon. The Achilles connects the gastrocnemius and soleus to the calcaneus (heel bone), transferring the contractile force of the calf muscles into mechanical movement at the ankle. The Achilles tendon is the final common pathway for virtually all plantar flexion force production, making it a critical structure in both performance and injury contexts.
Plantar flexion does not occur in isolation at the talocrural joint. It is frequently accompanied by some degree of inversion or eversion at the subtalar joint below, depending on the activity. During push-off in running, plantar flexion is combined with slight supination. During lateral cutting movements, plantar flexion may be combined with inversion, a mechanism for ankle sprains. Coaches who understand plantar flexion as part of a multi-joint kinetic chain can design more effective, injury-preventive programs.
What Are the Primary Plantar Flexion Muscles?
Gastrocnemius
The gastrocnemius is the largest, most superficial, and visually prominent muscle of the calf. It consists of two heads: the medial head (larger, arising from the medial femoral condyle) and the lateral head (arising from the lateral femoral condyle). Both heads course distally to combine with the soleus tendon to form the Achilles tendon, inserting onto the posterior calcaneus.
Key anatomical feature: The gastrocnemius is a biarticular muscle, meaning it crosses two joints: the knee and the ankle. This has profound implications for its function and for exercise selection.
Primary functions:
- Plantar flexion of the ankle, with maximum force production when the knee is extended
- Assistance with knee flexion (it is a weak secondary knee flexor, working alongside the hamstrings)
Fiber type composition: The gastrocnemius contains a higher proportion of fast-twitch (Type II) muscle fibers relative to the soleus. This makes it well-suited for explosive, high-force, brief-duration plantar flexion tasks, such as jumping, sprinting, rapid directional changes, and power-focused athletic movements.
The knee angle dependency: Because the gastrocnemius originates above the knee, its effective length is determined by both ankle and knee position. When the knee is extended (straight), the gastrocnemius is at an optimal length for producing plantar flexion force. When the knee is flexed beyond approximately 20 to 35 degrees, the gastrocnemius becomes slack at its proximal attachment, and its ability to contribute to plantar flexion force diminishes substantially.
Research has confirmed that neural drive to the gastrocnemius decreases as knee flexion increases, while soleus activation remains relatively constant regardless of knee angle.
This is why standing calf raises (performed with a straight knee) preferentially load the gastrocnemius, while seated calf raises (performed with the knee bent to approximately 90 degrees) preferentially load the soleus.
Training implications: The gastrocnemius responds best to heavier loads with lower to moderate repetitions, consistent with its fast-twitch fiber composition. A full range of motion through both the lengthened position (deep stretch at the bottom of a calf raise) and the shortened position (full plantar flexion at the top) produces the greatest hypertrophy stimulus.
A 2023 study in PLOS ONE found that calf training at longer muscle lengths (stretching the gastrocnemius at the bottom of the movement) produced 15.2% greater medial gastrocnemius hypertrophy compared to full range of motion, with an even larger advantage over training in shortened positions.
Soleus
The soleus is the largest plantar flexor by cross-sectional area, though it sits beneath the gastrocnemius and is only partially visible. It originates from the posterior surfaces of the tibia, fibula, and the fibrous arch connecting them, and inserts via the Achilles tendon onto the calcaneus.
Key anatomical feature: The soleus is a monoarticular muscle, crossing only the ankle joint. It has no attachment above the knee and no involvement in knee movement. This single-joint architecture is the defining functional difference between the soleus and gastrocnemius.
Primary functions:
- Plantar flexion of the ankle occurs across all knee angles, but is dominant when the knee is flexed
- Postural stabilization of the tibia over the fixed foot during standing
- Venous return assistance ("soleus pump"), helping push blood back toward the heart against gravity during lower limb activity
- Closed-chain control of the tibia during walking and running
Fiber type composition: The soleus contains a very high proportion of slow-twitch (Type I) muscle fibers, making it one of the most fatigue-resistant muscles in the human body. This composition is appropriate to its function: maintaining upright posture against gravity and providing sustained force during walking and running requires a muscle that can contract repeatedly for hours without fatiguing.
Closed-chain kinetics: When the foot is planted on the ground, soleus contraction in a closed kinetic chain does something counterintuitive: it drives the superior end of the tibia posteriorly, effectively contributing to knee extension. This function is relevant in clinical populations with weak quadriceps (the soleus can partially compensate for quad weakness), and in athletes where controlled tibial movement during deceleration is critical for ACL injury prevention.
Training implications: The soleus responds best to lighter loads with higher repetitions, consistent with its slow-twitch fiber composition. Extended time under tension is more important for soleus hypertrophy and endurance than matching the heavy loading typically used for gastrocnemius training.
Most coaches significantly undertrain the soleus because they default to standing calf raise variations that prioritize the gastrocnemius. Seated calf raises, bent-knee calf raises, and single-leg variations performed with the knee bent are the essential tools for targeted soleus development.
Plantaris
The plantaris is a thin, vestigial muscle with a small belly and an extremely long, slender tendon. It originates from the lateral supracondylar ridge of the femur, above the lateral head of the gastrocnemius, and its tendon runs between the gastrocnemius and soleus before inserting on the calcaneus.
The plantaris contributes weakly to plantar flexion and knee flexion. In practical terms, its functional contribution is minimal. Its clinical significance is greater: plantaris tendon rupture can occur in middle-aged recreational athletes (commonly called "tennis leg") and is sometimes confused with more serious calf or Achilles tendon injuries. The plantaris tendon is also used as a donor graft in reconstructive tendon surgery.
The muscle is absent in approximately 7-10% of the population, with no functional deficit resulting from its absence.
The Secondary Plantar Flexion Muscles
These muscles are primary movers for their named actions (toe flexion, foot inversion, eversion) but contribute secondary plantar flexion force as a byproduct of their anatomy and line of pull around the ankle.
Tibialis Posterior
The tibialis posterior is the deepest muscle in the posterior compartment of the lower leg. It originates from the posterior tibia, fibula, and interosseous membrane, and its tendon wraps around the medial malleolus to insert across the midfoot and forefoot.
Primary function: Foot inversion (turning the sole inward) and arch support. The tibialis posterior is the primary dynamic support of the medial longitudinal arch of the foot.
Secondary plantar flexion role: As the tibialis posterior's tendon wraps behind the medial malleolus, it pulls the foot both inward and downward, contributing a mild plantar flexion moment.
Clinical significance: Tibialis posterior dysfunction is extremely common, particularly in older adults and runners with flat feet. Weakness of the tibialis posterior leads to progressive arch collapse, hindfoot valgus (heel rolling inward), and a cascade of biomechanical problems that affect the knee, hip, and lower back. Tibialis posterior tendinopathy is one of the most common causes of medial ankle pain in middle-aged women.
Flexor Digitorum Longus
The flexor digitorum longus originates from the posterior tibia, courses behind the medial malleolus, and divides to insert into the distal phalanges of toes 2 through 5.
Primary function: Flexion of toes 2 through 5, assisting with grip on uneven surfaces, and stabilizing the longitudinal arch during the push-off phase of gait.
Secondary plantar flexion role: The course of its tendon produces a mild plantar flexion moment at the ankle as a secondary action.
Training note: Most conventional lower-body exercises do not specifically load the flexor digitorum longus. Barefoot training, toe-gripping exercises, and specific rehabilitation protocols for arch collapse or hammer toe correction are the primary means of addressing this muscle.
Flexor Hallucis Longus
The flexor hallucis longus originates from the posterior fibula, courses behind the medial malleolus in its own tendon sheath, and inserts into the distal phalanx of the big toe (first hallux).
Primary function: Flexion of the big toe, which is critical for the final push-off phase of gait (the "toe-off") and for balance during single-leg stance.
Secondary plantar flexion role: Similar to the flexor digitorum longus, its course behind the medial malleolus produces a secondary plantar flexion moment.
Clinical significance: Flexor hallucis longus tendinopathy is particularly common in ballet dancers and gymnasts who perform repeated forceful plantar flexion on pointed toes. It is also implicated in some presentations of medial ankle pain in runners.
Peroneus (Fibularis) Longus and Brevis
The peroneal muscles occupy the lateral compartment of the lower leg. The peroneus longus originates from the upper fibula and crosses beneath the foot to the first metatarsal and medial cuneiform. The peroneus brevis originates from the lower fibula and inserts at the base of the fifth metatarsal.
Primary functions: Foot eversion (turning the sole outward) and lateral ankle stabilization. The peroneals are the primary dynamic restraints against ankle inversion sprain.
Secondary plantar flexion role: Both peroneal tendons course behind the lateral malleolus, producing a secondary plantar flexion moment as they pull the foot downward and outward.
Clinical significance: Peroneal weakness is the most consistent finding in chronic ankle instability. Athletes with weak peroneals are significantly more susceptible to ankle sprains, and repeated sprains further weaken the peroneals in a negative feedback loop that eventually leads to chronic ankle instability. Peroneal strengthening through eversion exercises with resistance bands is foundational to ankle rehabilitation.
Muscle Summary Table
What Are the Most Common Plantar Flexion Imbalances?
Imbalance 1: Gastrocnemius Dominance with Soleus Weakness
This is the single most common plantar flexor imbalance in gym populations. Because standing calf raises feel heavier and produce more visible pump than seated variations, most self-directed training and many coached programs accumulate far more gastrocnemius volume than soleus volume.
How to identify it: Ask the client to perform a single-leg calf raise with a straight knee (tests gastrocnemius) and then with the knee bent to 90 degrees (tests soleus). A client with gastrocnemius dominance will often perform 15 to 20 clean reps with a straight knee but struggle to complete 10 with the knee bent. The asymmetry in performance between these two conditions confirms the imbalance.
Consequences:
- Compromised running economy and endurance, since the soleus contributes the majority of plantar flexion force during sub-maximal running speeds (because the knee is never fully extended during running gait)
- Increased Achilles tendinopathy risk, as the Achilles tendon is exposed to uneven loading
- Reduced postural stability, since the soleus is the primary ankle stabilizer in quiet standing
- Slower recovery between sprints or plyometric efforts, since the fatigue-resistant soleus is the workhorse for sustained activity
Correction: Program 2 to 3 seated calf raise sessions per week, separate from any standing calf work. Use lighter loads, higher reps (15 to 25 per set), and extended time under tension. A three-second eccentric (lowering phase) plus a two-second pause in the deep stretch position significantly increases soleus recruitment per rep.
Imbalance 2: Bilateral Asymmetry (Left-Right Difference)
A clinically meaningful difference in plantar flexion strength between sides is more common than most coaches realize, particularly among clients with a history of ankle sprains, lower extremity injuries, or prolonged single-leg loading.
How to identify it: Compare single-leg calf raise performance (reps to fatigue) and endurance (timed single-leg calf raise) between left and right sides. A difference of 10-15% or more in performance between sides warrants targeted unilateral correction.
Consequences:
- Asymmetric loading patterns that increase injury risk at the ankle, knee, and hip on the dominant side
- Compensatory movement patterns in squatting, running, and jumping that reduce efficiency and increase injury risk
Correction: Program unilateral calf work (single-leg standing and seated calf raises) with priority given to the weaker side. Do not allow the stronger side to compensate within bilateral movements. The FitBudd guide to unilateral training provides a framework for structuring asymmetry correction within a complete lower-body program.
Imbalance 3: Peroneal Weakness and Ankle Instability
Clients with a history of ankle sprains, particularly lateral sprains (the most common type), often present with weakened peroneal muscles. This is not simply a consequence of the sprain itself: the lateral ankle ligaments damaged in a sprain are closely associated with the peroneal tendons, and the resulting pain inhibition and altered movement patterns reduce peroneal activation during rehabilitation.
How to identify it: Manual resistance testing of ankle eversion or resistance-band eversion testing will identify weakness. Single-leg balance assessment on an unstable surface (e.g., a wobble board) compared with the unaffected side is a practical field test. Balance asymmetry of more than 30% between sides is a reliable indicator of compromised ankle stability.
Consequences:
- Chronic ankle instability and repeated sprain risk
- Compensatory movement patterns at the knee and hip
- Reduced push-off efficiency during running and change-of-direction movements
Correction: Progressive peroneal strengthening with resistance bands (ankle eversion in multiple positions), single-leg balance and proprioceptive training, and sport-specific agility work. Balance training on unstable surfaces is specifically effective for restoring neuromuscular control after ankle sprains.
Imbalance 4: Tibialis Posterior Weakness and Medial Arch Collapse
The tibialis posterior is the primary dynamic stabilizer of the medial longitudinal arch. When it becomes weak or dysfunctional, the arch flattens under load, the hindfoot rolls inward (overpronation), and the tibia internally rotates. This affects not only the foot and ankle but every joint in the kinetic chain above.
How to identify it: Observe heel alignment during a single-leg calf raise. If the heel tilts into valgus (rolling inward) during the rise, tibialis posterior weakness or dysfunction is likely. Flat feet under load, particularly when combined with medial ankle pain or shin splints, suggest tibialis posterior involvement.
Consequences:
- Plantar fasciitis through altered arch mechanics and increased fascial tension
- Medial tibial stress syndrome (shin splints) is caused by increased tibial rotation
- Patellofemoral pain syndrome occurs through excessive tibial internal rotation, increasing lateral patellar stress
- Tibialis posterior tendinopathy is a progressive condition that can become debilitating
Correction: Targeted tibialis posterior strengthening through resistance band inversion, progressive single-leg heel raises performed on a slight inversion bias, arch activation exercises, and potentially orthotic support while the tendon heals.
Imbalance 5: Overall Plantar Flexor Weakness (Bilateral Calf Deficit)
Some clients, particularly those new to training, sedentary individuals, or older adults, present with generalized weakness across all plantar flexor muscles. The clinical sign is an inability to perform 25 single-leg calf raises on either side, or visible collapse in form during calf loading.
Consequences:
- Reduced propulsive force during walking and running, leading to compensatory hip-dominant gait patterns
- Increased fall risk in older adults, since the calf complex is a primary contributor to reactive balance correction
- Limited athletic performance in any sport requiring explosive push-off or sustained lower leg endurance
Correction: Begin with bilateral standing and seated calf raises, progress to single-leg variations, and ensure adequate calf training volume across both gastrocnemius and soleus targets. Building a volume base of 10 to 15 direct calf sets per week is appropriate for correcting a significant bilateral deficit.
Best Exercises for Plantar Flexor Training and Imbalance Correction
Standing Calf Raise (Primary Gastrocnemius)
Setup: Stand on the balls of both feet on a raised platform (a step edge, a calf-raise machine footpad, or a weight plate). Heels hanging below the platform allow a full range of motion into the stretched position. Hold a support for balance or load with a barbell, dumbbell, or machine.
Execution: Lower the heels fully toward the floor to achieve a deep stretch. Pause for one second at the bottom. Rise onto the toes through the full range of plantar flexion. Pause for two seconds at the top. Lower under control.
Programming for gastrocnemius hypertrophy: 3 to 4 sets of 8 to 15 reps. Because the gastrocnemius contains more fast-twitch fibers, it responds to heavier loading and moderate rep ranges more than the soleus.
Key technique note: Research in 2023 confirmed that training in the lengthened position (deep stretch) produced up to 15% greater medial gastrocnemius hypertrophy than full range or shortened-position training. Prioritize the bottom stretch in every rep.
Seated Calf Raise (Primary Soleus)
Setup: Sit on a bench or a seated calf-raise machine with the knees bent to approximately 90 degrees. Place the balls of the feet on a raised platform. If using a machine, position the knee pad across the lower thigh. If using free weights, place a dumbbell or barbell across the lower thighs.
Execution: Fully lower the heels to achieve a stretch. Pause for two seconds. Push up onto the toes through a full range of plantar flexion. Pause at the top. Control the return.
Programming for soleus: 3 to 4 sets of 15 to 25 reps with a slow, controlled tempo. The soleus is slow-twitch dominant and responds best to extended time under tension rather than heavy loading. Rest periods of 60 to 90 seconds are appropriate, as the soleus recovers quickly between sets.
Single-Leg Calf Raise (Unilateral Assessment and Correction)
Purpose: Diagnoses and corrects bilateral asymmetry, doubles the mechanical load per limb without requiring additional external weight, and improves neuromuscular control at the ankle.
Straight-knee version: Targets gastrocnemius. Stand on one foot, with the ball of the foot on a raised surface, and hold a support for balance. Perform through the full range. Progress by adding load (dumbbell, weighted vest).
Bent-knee version: Targets soleus. Sit on a bench with knees at 90 degrees. Place one foot on a small platform and perform the raise with only that leg. Progress by adding a dumbbell across the thigh.
Peroneal Strengthening (Lateral Ankle Stability)
Resistance band eversion: Loop a resistance band around the forefoot. Sit with the leg extended. Ever the foot (turn the sole outward) against band resistance through a full range of motion. Hold two seconds at the end range. Return under control. 3 sets of 15 to 20 reps.
Standing resistance band eversion: Attach a band to a fixed point. Stand sideways and pull the foot away from the anchor (eversion) while maintaining a stable ankle. This more closely replicates the functional demand on the peroneals during movement.
Single-leg balance on an unstable surface: Progress from a firm floor to a foam pad to a wobble board. Begin with eyes open and progress to eyes closed to remove visual compensation. Start with 30 to 60 second holds and progress to dynamic tasks (ball catch, reaching).
Tibialis Posterior Strengthening
Resistance band inversion: Attach a resistance band to the forefoot. Sit with the leg extended. Invert the foot (turn the sole inward and upward) against resistance. Hold for two seconds. Return slowly. 3 sets of 15 reps.
Single-leg heel rise with inversion focus: Perform a single-leg calf raise while consciously shifting weight to the medial (inner) ball of the foot at the top of the rise. This recruits the tibialis posterior to stabilize the arch during the rise. Avoid heel valgus (rolling inward) throughout.
Programming Plantar Flexor Work Into a Training Plan
The calves and plantar flexors require different programming considerations than other muscle groups because:
The soleus needs different loading parameters than the gastrocnemius: Most coaches use a single calf exercise with a single-rep range, which optimally trains one muscle at the expense of the other. Effective programming includes both standing (gastrocnemius) and seated (soleus) variations with rep ranges matched to each muscle's fiber type.
High frequency is well-tolerated: The plantar flexors, particularly the slow-twitch soleus, recover quickly from moderate loading and respond well to twice or three-times-weekly training. Unlike large muscle groups, which require 48 to 72 hours of recovery after heavy sessions, the calves can be trained productively on consecutive days when loads are appropriate.
Volume requirements are higher than most coaches' programs: Ten to 15 direct working sets per week across both standing and seated variations is a reasonable target for clients seeking meaningful plantar flexor development or correcting an imbalance.
Eccentric loading is critical for the health of the Achilles tendon: it is most effectively loaded and strengthened through controlled eccentric (lowering) calf-raise work. Heavy-loaded eccentric calf raises (using both legs to lift, single leg to lower) are the gold standard for Achilles tendinopathy rehabilitation and prevention. Coaches integrating this protocol should use 3 to 4 sets of 15 reps, with a slow, controlled eccentric of 3 to 5 seconds per rep.
For coaches incorporating plantar flexor work within a complete lower-body training system, the FitBudd resource on strength and conditioning principles covers periodizing lower-extremity training across mesocycles to build the ankle and calf complex alongside the larger muscle groups. Integrating this work within a complete workout plan design framework ensures plantar flexor training is not an afterthought but a systematic component of every lower-body program.
Understanding how plantar flexion mechanics relate to the opposing motion provides additional programming context. The FitBudd guide to dorsiflexion vs plantar flexion explains how these two ankle motions function together in gait, athletic performance, and injury prevention.
Plantar Flexion Injuries Linked to Muscle Imbalances
Achilles Tendinopathy
Achilles tendinopathy is the most common calf-related injury in runners and athletes. It occurs when the Achilles tendon is subjected to repetitive loading that exceeds its adaptive capacity, leading to structural changes within the tendon and the characteristic pain and stiffness that define the condition.
The connection to plantar flexor imbalances is well-established: an undertrained soleus, which should bear the primary loading burden during running (since the knee is always slightly flexed during the gait cycle), forces the gastrocnemius and Achilles tendon to absorb disproportionate load. Over time, this creates cumulative tendon stress that exceeds the healing response.
Evidence-based treatment centers on heavy slow resistance training for the calf complex, specifically eccentric-concentric calf raises performed through a progressive loading protocol over 8 to 12 weeks. Coaches working with clients in rehabilitation contexts should be familiar with this protocol and coordinate closely with the treating physiotherapist.
Plantar Fasciitis
The plantar fascia is a thick band of connective tissue running along the bottom of the foot from the heel to the toes. Plantar fasciitis is an overload injury to this structure, typically presenting as sharp heel pain upon first rising in the morning.
The plantar flexor connection: tight, weak plantar flexors, particularly the gastrocnemius and soleus, reduce the ability of the calf complex to absorb ground reaction forces during heel strike. This transfers more energy to the plantar fascia. Tibialis posterior weakness allows arch collapse under load, further increasing fascial tension. Stretching the calf complex (particularly the gastrocnemius and soleus separately, since the knee-straight stretch targets the gastroc while the knee-bent stretch targets the soleus) is a first-line intervention because it directly reduces plantar fascial tension.
Calf Strains
Calf strains (particularly gastrocnemius tears at the medial head) are among the most common muscle injuries in team sport athletes. The medial gastrocnemius is the most frequently strained site due to the combined demands it faces as both a knee flexor and ankle plantar flexor during explosive movements.
Risk factors include inadequate soleus strength (creating over-reliance on the gastrocnemius), poor warm-up practices before explosive activity, and accumulated fatigue in athletes with high training loads.
Prevention involves adequate soleus and peroneal training, progressive plyometric loading, and year-round appropriate eccentric calf strengthening.
Ankle Sprains
Lateral ankle sprains are the most common acute sports injury. While they primarily involve ligamentous structures, peroneal weakness is the most important modifiable risk factor for both initial sprains and recurrence. Athletes with weak peroneals lack the rapid, reflexive eversion response needed to prevent the ankle from rolling into inversion during unexpected ground contact variations.
For a comprehensive look at how plantar flexion mechanics and ankle function connect across the full spectrum of movement, the FitBudd guide to plantar flexion: meaning, muscles involved, and why it matters for movement extends these concepts into gait mechanics and sport-specific contexts. Corrective approaches to the movement dysfunctions these injuries cause are covered in the FitBudd guide to corrective exercise, definition, examples, and uses.
Conclusion
Plantar flexion is powered by a sophisticated group of muscles with distinct anatomical properties, fiber type compositions, and functional roles. Understanding the difference between the gastrocnemius and the soleus, recognizing the contributions of the tibialis posterior and peroneals, and knowing how to assess and correct common imbalances separates coaches who prevent calf and ankle injuries from those who repeatedly refer clients to physiotherapy for the same recurring problems.
The practical takeaways are clear. Program both standing and seated calf raise variations. Train the soleus at higher reps with longer time under tension. Address peroneal weakness in any client with a history of ankle sprains. Test for bilateral asymmetry with single-leg assessments.
Train the eccentric phase with purpose, not just the concentric. And treat plantar flexor development as a systematic component of lower body programming rather than an accessory afterthought.
FitBudd makes it straightforward to build plantar flexor training and imbalance correction into every client's program, track session-by-session performance, and manage the complete coaching workflow in one platform. Start your free 30-day trial at FitBudd and deliver lower body programs built on anatomy, not assumptions.
%20to%20Become%20a%20Certified%20Personal%20Trainer-min.avif)








